
Top Docs 2011
Mr. Roboto
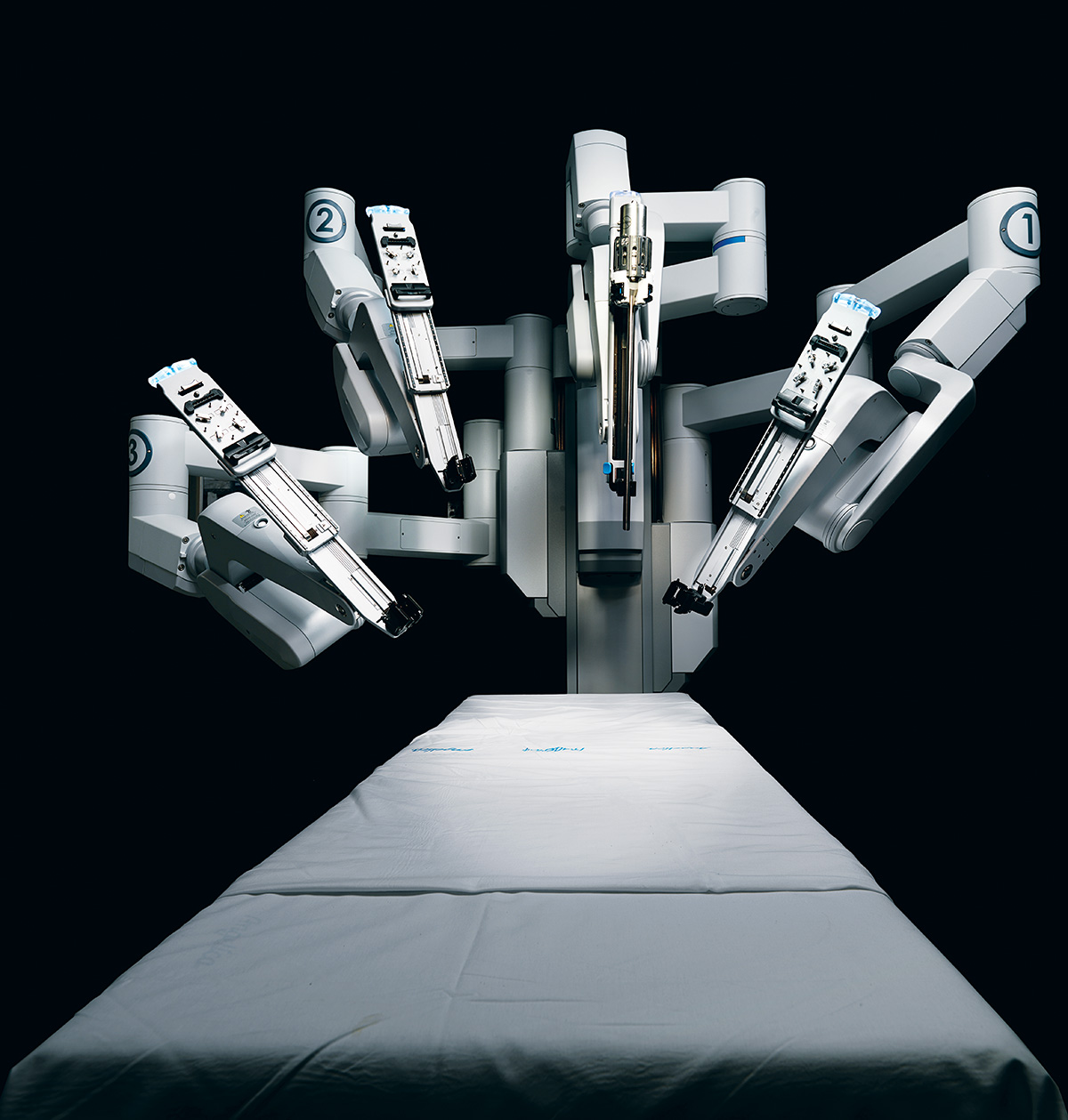
Photograph by Bruce Peterson
Sometimes having a big mouth can be good for your health. For patients with head and neck tumors, for instance, a spacious oral cavity can be the difference between a massive procedure that cuts through the jaw and throat, opening up the face like a book, or a minimally invasive surgery done with the help of a robot. At Boston Medical Center, otolaryngologists Gregory Grillone and Scharukh Jalisi have redefined the concept of “open wide” by perfecting a technique called transoral robotic surgery (TORS), recently approved by the FDA. When a patient has a relatively large jaw, doctors can remove tumors in hard-to-reach places — behind the tonsils and tongue, say, or deep in the larynx and throat — by using a remote console to maneuver several robotic arms, each outfitted with an HD camera or surgical tool. The robotic precision allows the doctors, who performed more than 30 of the operations this year, to better clean out tumors, and it gets patients home in days rather than weeks. — J.N.
The 10 Percent Doctrine
Doctors have long known that up to 10 percent of all heart attack patients die within a year; the problem was that they didn’t know which 10 percent were at risk. They do now, thanks to the work of Zeeshan Syed, who discovered the answer while in the joint health sciences doctoral program run by Harvard and MIT. Syed scanned the electrocardiogram readings of nearly 5,000 patients — tens of thousands of hours of recorded heartbeats — and discovered patterns, called biomarkers, that hospitals can now use to identify high-risk patients. “We can tease something out of nothing,” says Syed, who published his findings in September. You just have to look. — J.N.
A Current Affair

Illustration by Adam McCauley
One of the most challenging aspects of treating patients with ALS, or Lou Gehrig’s disease, is figuring out whether the treatments are working at all. That’s because patients are often too weak to endure the strength and breathing tests that measure the deterioration of their muscle function. The problem was maddening for Seward Rutkove, the neuromuscular disease chair at Beth Israel Deaconess Medical Center and a professor at Harvard Medical School. “I was obsessed with the idea that we needed new ways to evaluate muscle health,” Rutkove says. Years ago, he encountered the work of two Northeastern University physicists who were examining how muscle tissue responds to electrodes. Working alongside them, Seward developed a technique, electrical impedance myography (EIM), that determines a muscle’s condition by sending an imperceptible electrical current through it. EIM testing works on almost any muscle in the body, providing doctors with a quick way of knowing whether ALS medications are effective — a benefit that could cut the cost of medical trials in half. In February Rutkove was awarded a $1 million prize for his findings from Prize4Life, an organization that promotes and funds scientific innovation for treating ALS. With the prize money and a team of scientists from MIT, he’s developing a handheld EIM device that will give doctors newfound muscle in treating the disease. — J.N.
Your iPhone Will See You Now
Thanks to the work of Boston-area researchers, your smartphone just might save your life one day. When it comes to the following medical problems, there’s an app for that.
Diabetes
Northeastern University researcher Heather Clark and her team have developed what’s quite possibly the most badass blood test the disease has ever seen. It’s a tiny tattoo packed with a glucose-sensing dye that, when hit with a special light from your handy iPhone attachment, reveals your blood-sugar status. Bye-bye, finger pricks.
Tumors
New this year from Mass General: an app and a tiny machine that will take biopsies of miniscule tumors and analyze and summarize the results within an hour. That means no pathology lab, virtually no wait for results — and no invasive digging for samples. The hospital’s now at work on a smartphone blood test for cancer.
Mental Health
“You seem stressed, is everything okay?” It’s not a text from your mom, it’s a little smartphone counseling courtesy of the Daily Data app from MIT startup Ginger.io. Released this year, the app analyzes accelerometer data and the frequency of your calls, texts, and game-playing to monitor your mood (and even your chronic diseases).
Bogus Meds
Sproxil dealt a major blow to the $200 billion counterfeit-drug industry with a new app that sniffs out fake medicines. The Cambridge tech firm partnered with drug companies to put scratch-off codes on their packaging. Enter the code into the app, and a text will appear a few seconds later verifying the drug’s authenticity.
Cataracts
Last year, MIT’s Media Lab gave us the iPhone app for eyeglass prescriptions. This year, they developed a $5 iPhone app that can detect cataracts — and their spread and severity — earlier than even professionally trained specialists can find them. Oh, and the app can do it all in five minutes or less. — S.F.
Putting Doctors on the Clock
Earlier this year, two Harvard Business School professors had a thought. What if, instead of relying on arbitrary estimates from Medicaid or Medicare, hospitals could determine what healthcare procedures actually cost? To find out, they asked two Boston surgeons to introduce a new tool to their medical kits: a stopwatch.
Professor Robert Kaplan’s theory, “Time-Driven Activity-Based Costing,” has been used by businesses across the country to help track efficiency and outcomes. But it’s never been tried in a hospital setting, in part because we prefer our doctors to focus on saving lives rather than worrying about the cost of care. But that’s left a huge gap in understanding, says Kaplan’s colleague, Michael Porter, who has researched healthcare delivery for more than a decade: “It’s not because of how physicians are trained. They’ve just never had any way of knowing or thinking about it.”
The professors launched a pilot program, recruiting John Wright, who performs knee replacement procedures at Brigham and Women’s, and John Meara, who runs the cleft palate unit at Children’s Hospital, to take part. The doctors asked their staffs to help them map out each step in a patient’s treatment, from the moment they’re checked in at the door of the hospital to their final follow-up visit. A per-minute cost was then calculated based on the time that each doctor, nurse, clinician, or assistant spent with the patient. Then all of the overhead costs were factored in — equipment, electricity, cleaning and sanitizing of tools — and were added up to create a full cycle of care.
Mapping the process allowed the doctors to identify inefficiencies, like the amount of time nurses spent filling out paperwork instead of tending to patients. And it enabled them to look at how well their patients fared relative to how much money was spent on their care. In one example, Meara found that when it comes to cleft palates, 40 percent of the costs incurred over 18 months of care stemmed from the few days a child spent in the ICU after surgery. He then determined that the same child could, with just a bit of extra oversight, recover equally well in a less-expensive general wing of the hospital. For his part, Wright learned that an exercise machine used to strengthen the knee after surgery was actually detrimental to patients. So he transferred the cost of the machine to more physical therapy, and his patients wound up recovering faster.
Could these results lead to an entirely new financial plan for hospitals? It’s too early to know for sure, but the business professors’ cost-mapping idea has proven to be a valuable start. “We’re spending too much money and we’re not sure whether we’re getting the value for it,” says Wright. “We can’t afford to continue to run the system as we are.” — J.N.
HIV-Free
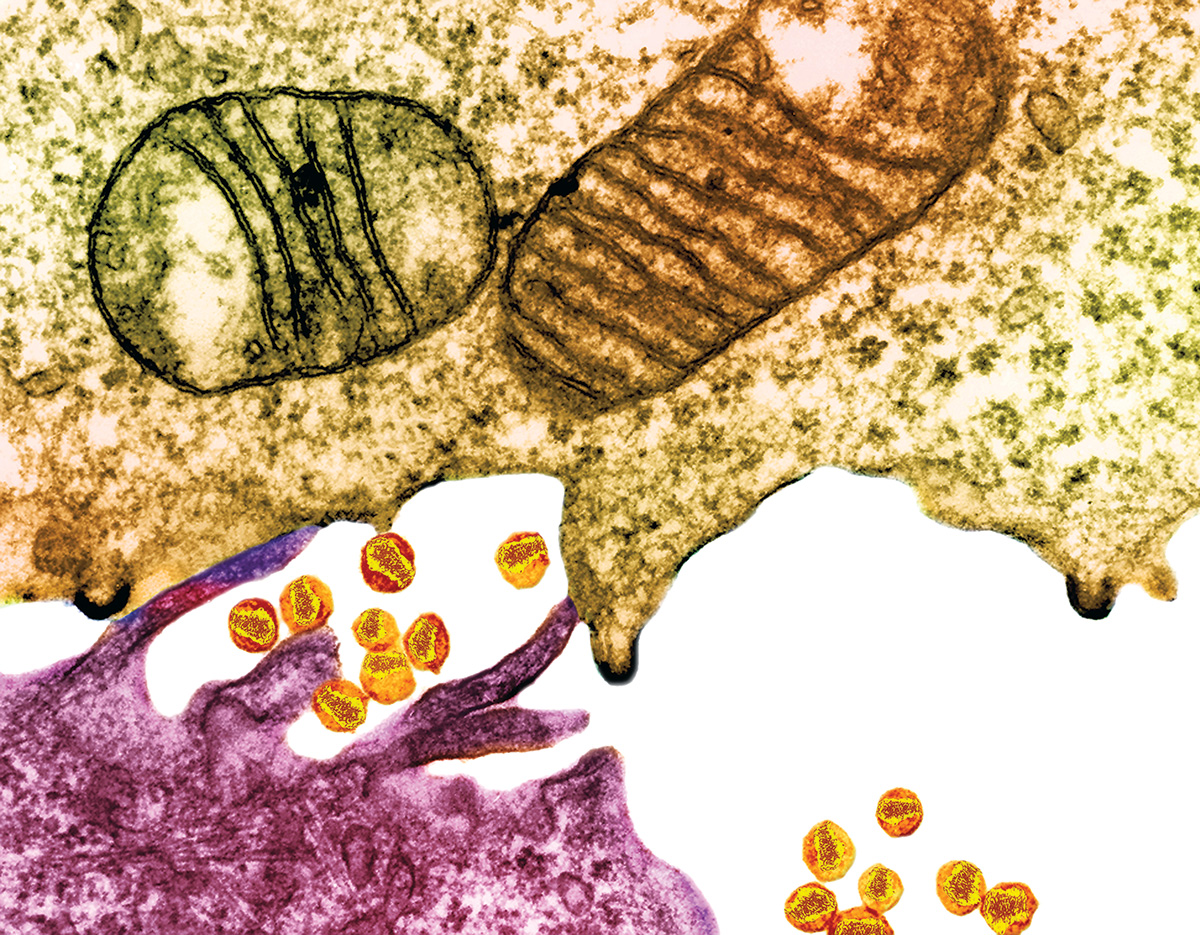
Photograph by David Phillips/Visuals Unlimited
An HIV vaccine has remained elusive for decades, in part because just when researchers think they have it pinned down, the wily virus mutates and slips away. As MIT immunologist Arup Chakraborty observes, HIV is so protean that a single infected person can have as many strains of the virus in his body as there are annual strains of flu in the entire world. But now Chakraborty and Harvard Medical School’s Bruce Walker may be closing in on the virus’s undoing. Chakraborty looked beyond the constantly changing individual proteins in the virus, and instead focused on identifying groups of proteins that weren’t mutating as much. It was there, he reasoned, that you would find HIV’s basic structures. Attack one of those structures at various points, and the virus would actually harm itself when it mutated.
Chakraborty identified one of these “polyproteins” through computational analysis, which Walker then confirmed by testing a group of long-standing HIV patients. They published their findings in June, and animal trials will begin in a few months. Chakraborty began work on HIV just three years ago, after he joined Walker — who has studied the virus since the ’80s — on a visit to South Africa’s AIDS-ravaged KwaZulu-Natal province. The pair now work collaboratively through the Ragon Institute, a consortium formed by MIT, Harvard, and Mass General. Producing a vaccine is not only urgently needed, but it may be the only viable solution, says Chakraborty. “Monitoring and treatment through therapy is difficult in the sub-Saharan region, where you might have one clinic and five nurses for half a million people.” — Matthew Reed Baker
Can You See Me Now?

Photograph by Bruce Peterson
If you think Siri and location-based apps make your life easier, just imagine what the technology can do for the sight-impaired. Joseph Rizzo III, the director of neuro-ophthalmology at Mass Eye and Ear, and his team have developed a prototype for “smart” glasses that guide the blind around unfamiliar environments. Here’s how they’ll work. — Courtney Hollands
1) Audio cues identifying objects around the wearer are sent to an earpiece.
2) Small vibrators placed at the temple and the back of the ear buzz when the patient needs to turn or avoid an object.
3) A camera embedded in the glasses captures and sends images to a small GPS-enabled processor, which identifies objects and people and “reads” signs and text via optical character recognition.
It’s All in the Genes

Illustration by Adam McCauley
Patients have typically had two options for attacking cancer: surgery or chemotherapy. But now, thanks in part to the work of a team of researchers at Dana-Farber Cancer Institute, we may be at the dawn of a new era of treatment. The researchers have come up with “smart medicines,” or molecular-targeted therapies, that attack certain genetic defects in patients that can cause cancerous tumors.
These particular cancers are fed by proteins gone haywire. The smart meds turn off those proteins, cutting off the tumor’s food supply and causing it to die. Success rates in clinical trials have been startlingly high. In one instance, a woman named Beverly was diagnosed with late-stage lung cancer and given six months to live. Then Pasi Jänne, associate professor of medicine at Dana-Farber, discovered that Beverly’s lung cells contained an alteration in a protein called anaplastic lymphoma kinase (ALK), a mutation that produces rapidly growing tumors in 5 percent of non-small-cell lung cancer patients. Jänne enrolled her in a clinical trial of a new drug, crizotinib, that essentially acts as a kill switch for ALK.
Within six weeks, Beverly’s tumors had shrunk by more than half. Where chemo typically has an efficacy rate of 30 to 40 percent for cancers like this, with smart medicines it’s more like 70 to 80 percent. “When they work, they usually work in days,” Jänne says, “not in weeks or months that we see with chemotherapy.” The FDA approved crizotinib in August, and other smart medicines are in the works for certain types of melanoma and leukemia. — Casey Lyons